In the UK, one man in five dies before he reaches 65. Together we can change that. Donate, sign up for news or order some of our man manuals from the online shop.
Related content

Make the promise. Stand up to male violence.
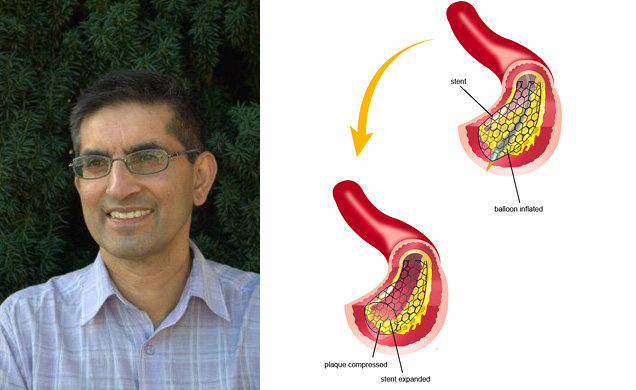
Mehboob: 'my heart attack will make me a better doctor'
I went to the gym just round the corner as usual. I go nearly everyday. We do a work-out of the day at 4pm when we exercise together. There were only three guys there. A football player, a rugby player, all in their early 20s. I should have thought twice. We did a big routine: 30 kettle weights, 30 press-ups, 30 squats, 30 burpees. We repeated it three times. The other guys were all sweltering and were amazed I’d managed to keep up. So was I.
I thought I'd pulled a muscle
I had a hot shower. As I got in the car, the pain began. By the time I got home, I was only holding the steering wheel with one arm and poking around at my chest. It was quite tender. I thought I’d pulled a muscle or hurt my ribs. But when I arrived home, my wife Liz got me some anti-inflammatories and called the ambulance. Luckily, it arrived within seven minutes. As a doctor I was trying to work out what was wrong. I get indigestion and thought it may be that.
I wasn’t improving, yet I wasn’t convinced it was a heart attack until I saw the ECG the paramedics did. I couldn’t believe it was me. This was what I was used to seeing in my patients.
We have 24-hour stenting here. [A stent is a tiny wire mesh tube inserted into an artery to keep it open and prevent plaque from closing it up.] Stenting [angioplasty] is the definitive treatment for a heart attack these days. I had two in within two hours. One of my colleagues did it. The nurse was a former patient. ‘What are you doing here?’ she asked.
I was low on the risk factors
I was a bit euphoric at this stage. Chatting away. It hadn’t sunk in. I felt as if I was watching a movie. After the surgery, alone in bed, I began to realise. You feel pretty vulnerable as a patient. I couldn’t even go to the loo. It was quite sobering.
I was low on all usual risk factors like blood pressure and cholesterol. Waist is 90-91cm [just under 36 inches]. My Body Mass Index (BMI) was perhaps slightly over. Usually up to 25 is considered OK but for Indians some doctors think you should revise it down to 23. Mine is 23.5. My cardiologist told me half of the heart attacks around the world are in the Indian population.
I know from the literature that there’s a good chance of getting depressed after a heart attack so I’ve focussed on the positives. The week-end before I’d been camping with my family on an island. If it had happened there… Well, I figure I’ve been given a second chance. The atherosclerosis [the build-up of fatty plaque which can cause a blockage inside the arteries] must have been there for a while and at least it has now been picked up.
I had a couple more stents added next day as I was getting signs of angina. They put me on a treadmill the day after my heart attack! So I have four stents now and take six tablets everyday.
Chronic stress can cause inflammation
I take it easy. I need to recover. I hope to get back to doing what I was doing before and it might be easier as the blockage is now unblocked. It’s very humbling.
I think it will help me be a better doctor. I’ve treated people with heart attacks but you feel it’s never going to happen to you. Up until now I’ve always been so well.
Inflammation is the basis for a lot of health issues including cancer and heart disease. Chronic stress can play a big part in inflammation and increase the risk of atherosclerosis. I don’t feel stressed. I’ve always used stress as a motivator. Indeed, I've enjoyed being calm in stressful situations. But I wonder now if doing this regularly has been bad for me. It’s a bit like drinking. You may feel mentally OK afterwards but you don’t know how your body is reacting. I’ll never know the answer. Would I have got this problem with a different lifestyle?
Some people who have had them a while talk about stents as if they’re minor, everyday things and I wonder if I'll get to have that attitude. I’m doing a mindfulness course. I’d started it before the heart attack. I find it helpful. There are lots of benefits in the medical literature so I thought I’d give it a go. We have so many stories going around inside our head and they’re not reality, they’re just thoughts. Why be bothered with them? Focus on the now. I keep bees and they’re very mindful. I just love watching them.
What about the NHS?Mehboob lives in New Zealand and that is where he had his heart attack. But what would have happened to him in the UK on our NHS? The key measure to answer this question is the so-called 'call to balloon' time (CTB): the time between alerting emergency services (999) and the start of treatment to reopen the blocked artery. The research suggests that in 2015/16, 80% of NHS patients had a CTB of under two and a half hours (150 minutes) - the national target - with a little over half getting treatment within two hours like Mehboob. There is evidence that treatment time, once inside the hospital is improving, but nevertheless overall CTB times have increased slightly (by 10 minutes between 2010-11 and 2015-16) suggesting that travel times to hospital and/or time waiting for an ambulance have increased. The research appears in the Myocardial Ischaemia National Audit Project (MINAP) report carried out by the National Institute for Cardiovascular Outcomes Research. |
| This article reflects the experience of the individual. It is not health information from the Men's Health Forum under the terms of the NHS England Information Standard. |
|
The Men’s Health Forum need your support It’s tough for men to ask for help but if you don’t ask when you need it, things generally only get worse. So we’re asking. In the UK, one man in five dies before the age of 65. If we had health policies and services that better reflected the needs of the whole population, it might not be like that. But it is. Policies and services and indeed men have been like this for a long time and they don’t change overnight just because we want them to. It’s true that the UK’s men don’t have it bad compared to some other groups. We’re not asking you to ‘feel sorry’ for men or put them first. We’re talking here about something more complicated, something that falls outside the traditional charity fund-raising model of ‘doing something for those less fortunate than ourselves’. That model raises money but it seldom changes much. We’re talking about changing the way we look at the world. There is nothing inevitable about premature male death. Services accessible to all, a population better informed. These would benefit everyone - rich and poor, young and old, male and female - and that’s what we’re campaigning for. We’re not asking you to look at images of pity, we’re just asking you to look around at the society you live in, at the men you know and at the families with sons, fathers and grandads missing. Here’s our fund-raising page - please chip in if you can.
|