In the UK, one man in five dies before he reaches 65. Together we can change that. Donate, sign up for news or order some of our man manuals from the online shop.
Related content

Make the promise. Stand up to male violence.
Prostate FAQs
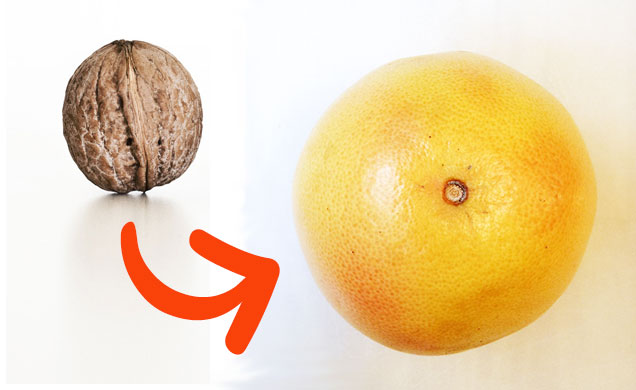
About the size and shape of a walnut, it is sited below your bladder and above the base of your penis, between your pubic bone and your rectum. It encircles the urethra (the tube through which urine passes from the bladder).
How it develops
- In newborn boys the prostate is about the size of a pea. It grows very slowly until puberty.
- Then it doubles in size in a dramatic growth spurt.
- When a man reaches his 40s it begins to increase in size again and can become as large as a grapefruit.
- Various hormones control its growth and function. The most important is the male sex hormone, testosterone.
Signs of a problem
The most common sign of a prostate problem is difficulty in passing urine. Changes in the prostate narrow the urethra, the tube which carries urine from the bladder.
You might experience:
- a weak flow
- intermittency — a flow which stops and starts
- hesitancy — having to wait before you start to go
- frequency — having to urinate more often than previously
- urgency — finding it difficult to postpone urination
- nocturia — having to get up at night to urinate
What do I do if I have symptoms?
Go to your GP. They may want to examine your prostate. This involves inserting a gloved finger into your anus to feel the size and shape of your prostate. They may also want to do a blood test.
What is the blood test for?
The blood test measures something called Prostate Specific Antigen (PSA). PSA is a protein produced by normal cells in the prostate and also by prostate cancer cells. It is normal for all men to have a small amount of PSA in their blood. A raised PSA level may show that you have a problem with your prostate, but not necessarily prostate cancer.
What can go wrong with my Prostate?
There are generally three conditions that affect the prostate.
- prostate enlargement
- inflammation of the prostate gland (prostatitis)
- prostate cancer
Prostate enlargement is a common condition associated with ageing. About a third of all men over 50 years of age will have symptoms of prostate enlargement. If the prostate becomes enlarged it can place pressure on the urethra, making it more difficult for the bladder to empty.
A simple treatment for prostate enlargement is to reduce the amount you drink before you go to bed.
Medications, such as alpha blockers, are also available to help relax the prostate gland muscles, or reduce its size, making it easier to urinate.
In more severe cases that fail to respond to medication, the inner part of the prostate gland that is blocking the urethra can be surgically removed using laser surgery. There also other less-invasive procedures to, for example, stop the prostate growing or from causing an obstruction
Research into the best surgical techniques continues with doctors looking for maximum effectiveness and minimum side-effects. In September 2015, NICE approved the UroLift technique which rather than cutting parts of the prostate away uses small implants to prevent the prostate pressing against the urethra (pee-tube) and making peeing difficult. Research into other techniques continues too.
Prostatitis is a poorly understood condition where the prostate gland becomes inflamed (red and swollen). Inflammation often occurs as a response to infection, but in most cases of prostatitis no evidence of infection can be found. Prostatitis is thought to affect up to 3 in 20 men (15%) at some point in their lives. Although it can affect men of any age, it is more common in men between 30-50 years of age. Prostatitis can be treated using a combination of painkillers and a type of medication known as an alpha-blocker, which can help relieve the symptoms.
Prostate cancer is the most common type of cancer in men, with over 40,000 new cases diagnosed every year. Your chances of developing prostate cancer increase with age. Most cases occur in men who are 50 years of age or older. The causes of prostate cancer are unknown, but risk factors include age, ethnic origin and family history.
The outlook for prostate cancer is generally good because, unlike many other types of cancer, it usually progresses very slowly. Many men die with prostate cancer, rather than as a result of having it.
If treated early, prostate cancer can often be cured. Treatments include:
- surgery to remove the prostate gland
- radiotherapy - using radiation to kill the cancerous cells
- hormone therapy - using medication to block the effects of testosterone (the hormone that stimulates prostate cancer)
Prostate Specific Antigen (PSA) is a chemical produced normally by prostate cells. It is a type of chemical known as an enzyme, and it is believed to have a role in liquefying semen after ejaculation (which may help in sperm motility).
PSA is only produced by prostate cells (it is prostate specific), but is produced by both cancerous and non-cancerous prostate cells (it is not cancer specific). Although PSA is the best example we have of a marker for prostate cancer this non-specificity for cancer means that there are reservations about the interpretation of raised values.
Essentially, one of the following scenarios may commonly occur:
· A man with prostate cancer may not have a raised PSA test (this is known as a false-negative result)
· A man with a raised PSA may not have prostate cancer (this is known as false-positive result)
The recent introduction of age-specific ranges for normal PSA values was an attempt to make the PSA test a better one. Rather than use the absolute limit of more than 4 ng/ml most urologists now use the following values:
Age (Years) Reference Range (ng/ml)
40-49 <2.5
50-59 <3.5
60-69 <4.5
70-79 <6.5
- See more at: http://www.malehealth.co.uk/prostate/19211-other-questions-cancer-and-ot...
Further Information
MAIN IMAGE from: PA263161 by Joy and A Walnut Story by Ivan licensed under CC BY 2.0.
We don't currently post comments online but are always keen to hear your feedback.
Date published
03/04/14
Date of last review
19/11/20
Date of next review
19/11/23
References
|
The Men’s Health Forum need your support It’s tough for men to ask for help but if you don’t ask when you need it, things generally only get worse. So we’re asking. In the UK, one man in five dies before the age of 65. If we had health policies and services that better reflected the needs of the whole population, it might not be like that. But it is. Policies and services and indeed men have been like this for a long time and they don’t change overnight just because we want them to. It’s true that the UK’s men don’t have it bad compared to some other groups. We’re not asking you to ‘feel sorry’ for men or put them first. We’re talking here about something more complicated, something that falls outside the traditional charity fund-raising model of ‘doing something for those less fortunate than ourselves’. That model raises money but it seldom changes much. We’re talking about changing the way we look at the world. There is nothing inevitable about premature male death. Services accessible to all, a population better informed. These would benefit everyone - rich and poor, young and old, male and female - and that’s what we’re campaigning for. We’re not asking you to look at images of pity, we’re just asking you to look around at the society you live in, at the men you know and at the families with sons, fathers and grandads missing. Here’s our fund-raising page - please chip in if you can.
|